
If your knee has ever caught, stuck, or refused to straighten, you know how unsettling it feels. One moment you are moving normally, the next your joint seems to jam. While some episodes are caused by stiffness or pain-related muscle guarding, true knee locking is often linked to a mechanical problem inside the joint. It is usually a mechanical block inside the joint. If you are searching for locked knee joint treatment, you are likely looking for clear answers about what causes this, whether it needs urgent attention, and what your options are. We help you understand exactly what this means, how we investigate it, and the steps we take to restore smooth, pain-free movement.
That Sudden Stuck Feeling: Understanding a Knee That Locks
Many people describe their knee as clicking, crunching, or giving way. These sensations are common and often harmless. A true mechanical lock feels different. It is a physical barrier that stops your knee from moving fully, usually when you try to straighten it. You may feel a sharp catch, or your joint may simply refuse to move past a certain point.
What locking actually feels like versus normal knee noises
A knee joint crunching sound, medically called crepitus, is very common. It often happens when you climb stairs or stand up from sitting. If there is no pain or swelling, this noise alone rarely requires intervention. Mechanical locking is different. It involves a tangible obstruction. You might feel your knee getting locked in place, needing to gently wiggle or shift your weight to release it. Recognising this distinction helps us choose the right path forward.
Mechanical lock versus pseudo-lock: why the difference matters
A pseudo-lock happens when pain or muscle spasm makes you avoid moving your knee fully. The joint itself is not physically blocked. A true mechanical lock means something inside the joint, like a torn piece of cartilage, is physically preventing movement. This difference is crucial because a mechanical block rarely resolves with rest alone and often requires specialist assessment.
Quick self-check: can you gently straighten your knee?
If your knee feels stuck, try this gentle check. Sit with your leg supported. Slowly try to straighten your knee. If you feel a hard, physical stop accompanied by catching, this suggests a mechanical block. If you can straighten it but it feels tight or painful, it may be pseudo-locking. Noting this early helps us focus our assessment efficiently.
Why locking happens suddenly, even without a major injury
You do not need a dramatic sports injury for your knee to jam. Sometimes a simple twist, a deep squat, or even standing up can cause a pre-existing tear to displace. Think of it like a doorstop suddenly jamming a door. The fragment was already there, but a specific movement flipped it into a blocking position. Understanding why knee locking problems occur in this way often removes the fear that you have caused new damage. We frequently hear patients ask why does my knee keep clicking alongside locking. Clicking alone is often benign, but when it progresses to actual jamming, it signals a mechanical shift that we investigate closely.
Common Causes Behind Mechanical Knee Locking
Understanding the exact cause is the foundation of effective care. The most common reasons involve structures inside your knee joint becoming displaced or damaged.
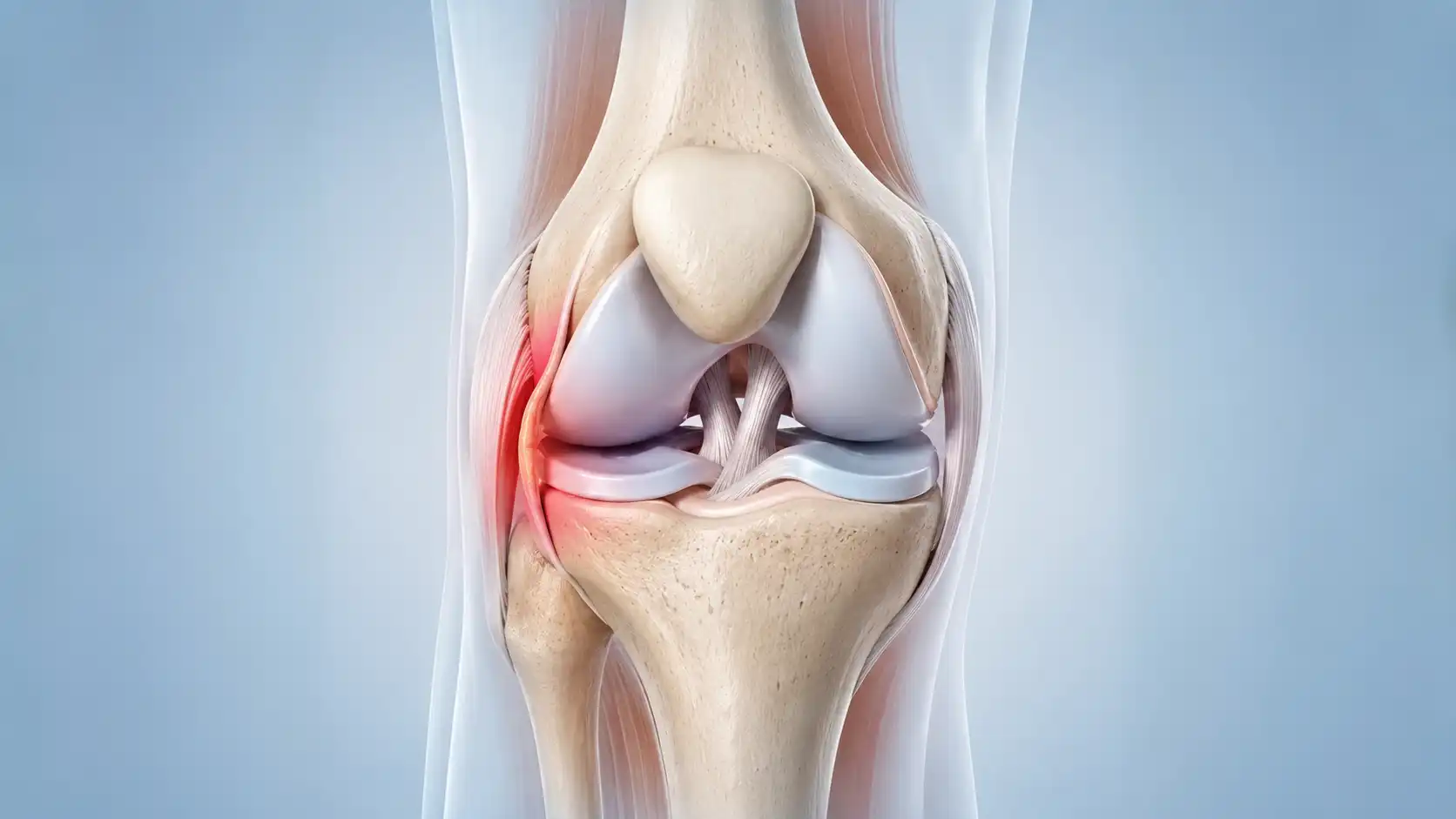
Bucket handle tear of meniscus: when cartilage flips and blocks movement
The meniscus is a C-shaped piece of cartilage that acts as a shock absorber. A bucket handle tear of meniscus is a specific type where a long fragment flips into the centre of the joint, much like a bucket handle. This displaced piece physically blocks the knee from straightening fully. It is one of the most frequent causes we treat, particularly in active individuals.
Why early assessment matters
- A displaced bucket handle tear may become harder to repair if left untreated.
- Early assessment improves the chance of preserving the meniscus.
- Delaying treatment may increase cartilage wear inside the joint.
- Some patients mistakenly wait for symptoms to settle, only to find locking episodes become more frequent.
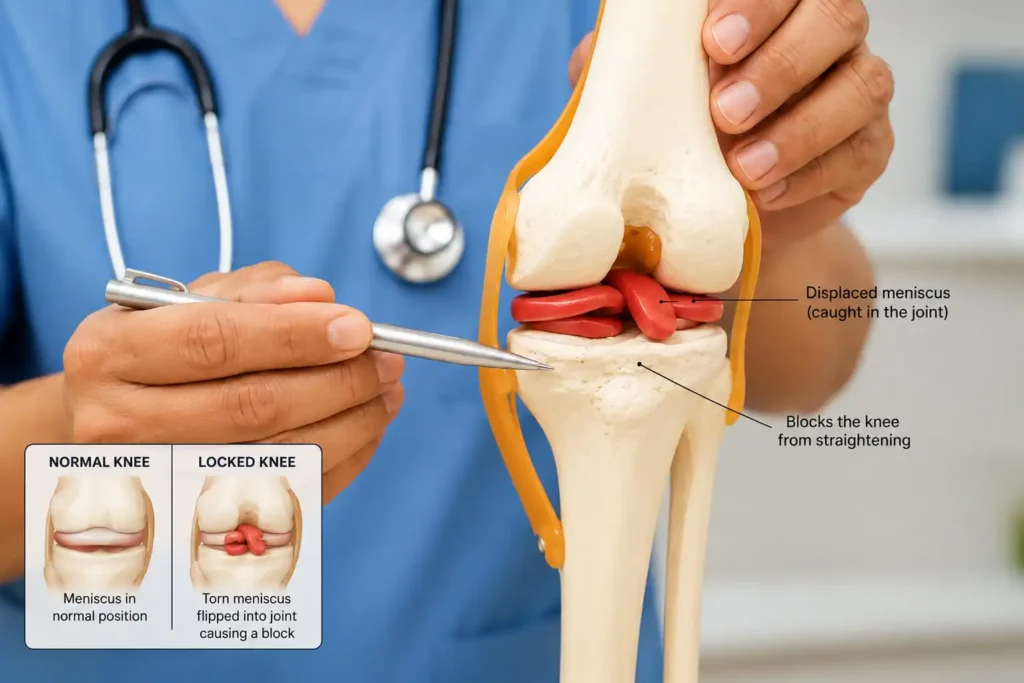
Why this tear causes a true mechanical block
The flipped fragment sits directly between the thigh bone and shin bone. When you attempt to straighten your leg, the fragment gets trapped. This creates the classic presentation where your knee that locks will not pass a certain angle until the fragment shifts. Addressing this promptly protects the surrounding cartilage.
Loose body in knee joint: how fragments create sudden locking
Sometimes small fragments of bone or cartilage break away and float freely inside the joint. A loose body in knee joint can drift into the moving parts and act like a pebble in a hinge. One moment your movement is smooth, the next the fragment catches. These fragments often come from previous injuries, wear and tear, or benign joint lining changes.
Other causes we consider: cartilage flaps, alignment issues and scarring
Other conditions can also cause jamming. A knee keeps locking when bent is a pattern we often link to posterior meniscus tears or cartilage irregularities at the back of the joint. If your knee is stuck at a very specific angle, such as a knee locked at 30 degrees, it is a classic clinical sign that helps us identify the exact location of the fragment or scar tissue. We also evaluate conditions like cyclops lesions (scar tissue following prior ligament surgery) or chondral flaps that catch during specific movements.
Can Knee Locking Happen With Age-Related Wear?
Yes. Knee locking is not limited to sports injuries or younger people. As we age, the meniscus naturally becomes less flexible and more prone to wear. Over time, small degenerative tears can develop gradually, sometimes without a specific injury or memorable event.
Unlike traumatic meniscus tears, which often occur after a twist or sudden movement, degenerative tears may develop slowly through everyday activities. Many people first notice occasional catching, clicking, or brief episodes where the knee feels as though it is not moving smoothly.
In some cases, a worn or frayed section of meniscus can become unstable and catch between the moving surfaces of the joint. This can create symptoms similar to a mechanical lock, including pain, catching, or difficulty fully straightening the knee. Degenerative cartilage changes and early osteoarthritis can also contribute to these sensations.
Understanding the difference between a traumatic tear and age-related wear is important because treatment recommendations may vary. While some degenerative tears can be managed successfully with physiotherapy, activity modification, and strengthening exercises, persistent locking symptoms should always be assessed to identify the underlying cause and determine the most appropriate treatment plan.
Signs That Age-Related Meniscus Wear May Be Contributing
You may be experiencing a degenerative meniscus problem if:
- Symptoms developed gradually rather than after a specific injury.
- You are over the age of 40.
- The knee catches or clicks during everyday activities.
- Pain is worse after prolonged walking or standing.
- Locking episodes become more frequent over time.
- You also experience stiffness, particularly in the morning or after sitting for long periods.
Symptoms That Suggest You Need Locked Knee Joint Treatment
Not every ache or click means you need a procedure. However, certain patterns strongly suggest a mechanical problem that benefits from specialist review.
Key signs it is a mechanical lock, not just stiffness
Look for these indicators. You feel a definite physical stop when trying to move your joint. The jamming happens at a specific angle. You may notice swelling after activity. Experiencing a knee giving way and painful sensations together often points to a mechanical catch that suddenly shifts, briefly destabilising your leg. These symptoms together guide us toward a targeted approach.
When locking happens with specific movements
Pay close attention to your triggers. Knee locking when bending often points to a problem at the back of the joint space. If you notice your knee locks back when walking, it may relate to how your leg aligns during your natural stride. Tracking these patterns allows us to narrow the diagnosis quickly during your consultation.
Red flag symptoms: when locking needs urgent attention
Most episodes are not medical emergencies, but certain signs warrant prompt evaluation. If knee locking passing out occurs due to a sudden pain spike or vasovagal response, it indicates a severe mechanical irritation. We advise seeking same-day assessment if you have a hot, swollen knee with fever, cannot bear any weight, or experience numbness below the joint.
If these signs appear, please do not wait. We can assess this quickly and help you avoid unnecessary strain or further tissue irritation.
Signs to seek same-day assessment
Contact our team urgently if you have severe swelling after a recent twist or fall, your joint will not straighten at all despite gentle attempts, or you show signs of infection. Early evaluation protects your long-term joint health.
How We Diagnose the Cause of Your Locked Knee
Accurate diagnosis is the foundation of everything we do. Our assessment begins with listening carefully to your experience and examining how your joint moves under different angles.
What to expect when you see us
Your appointment focuses on your daily life and specific symptoms. We ask when the jamming started, what movements trigger it, and how it affects your routine. Our lead consultant will then perform a hands-on examination, gently moving your knee through its full range to feel for catches, instability, or tender areas. This clinical evaluation often reveals more than scans alone.
Imaging that reveals the hidden cause
When a mechanical block is suspected, we usually recommend an MRI. This scan provides detailed pictures of your soft tissues, including the meniscus, ligaments, and cartilage surfaces. A weight-bearing X-ray may also be used to assess your bone alignment and joint space. Together, these images give us a complete picture of what is happening inside.
Why MRI is often essential
Standard X-rays show bone beautifully but cannot visualise cartilage or ligaments. An MRI reveals soft tissue tears, loose fragments, and scar tissue clearly. This precision allows us to plan a targeted intervention rather than guessing. In cases of a true locked knee, MRI is often arranged urgently because identifying a displaced meniscal fragment early may influence treatment options.
When X-rays still matter
X-rays remain a vital baseline. They show joint spacing, alignment, and any underlying bone changes that might influence your treatment plan. Using both tools ensures we never miss a contributing factor.
Clinical tests that pinpoint mechanical blocks
During your examination, we perform specific movement tests to reproduce your symptoms safely. We check for joint line tenderness and assess how your kneecap tracks. These skilled examinations, combined with your imaging, lead to a confident diagnosis. We guide you on the next steps once we know exactly what we are dealing with, ensuring you never feel rushed or uncertain.
Treatment Options: From Guided Rehab to Keyhole Surgery
The right path depends entirely on your diagnosis, your activity goals, and the overall health of your joint. Our approach always starts with joint preservation.
When non-surgical care may help
If your jamming is mild, intermittent, or linked to muscle imbalance, physiotherapy and load management often provide excellent results. We focus on strengthening the muscles that support your joint to improve stability. Learning how to prevent knee locking involves targeted exercises, activity modification, and sometimes temporary bracing to allow inflammation to settle.
What conservative care actually involves
Conservative treatment is active, not passive. It includes specific strengthening routines, mobility work, and advice on managing flare-ups. The RICE protocol helps settle acute swelling, while gradual loading rebuilds confidence. This pathway is ideal for muscle-related catching or as a first step before considering procedures.
Keyhole surgery: why arthroscopy is the gold standard
When imaging confirms a true mechanical block caused by a displaced meniscus tear, loose body, or other obstructing tissue, arthroscopy is often the most effective treatment option. This minimally invasive procedure uses tiny incisions and a small camera to visualise and treat the problem directly. We can repair torn tissue, remove obstructing fragments, and smooth rough cartilage in one precise session.
What happens during the procedure
You are comfortably asleep under anaesthetic. We make two small portals, insert the camera and specialised instruments, and address the exact cause we identified on your MRI. Most patients go home the same evening with simple wound care instructions.
Meniscus repair versus removal: our joint preservation approach
Whenever anatomy allows, we prioritise repairing torn tissue rather than removing it. Preserving the meniscus maintains your natural shock absorption, which is vital for long-term joint health. If a fragment cannot be safely repaired, we carefully trim only the unstable portion. We always explain the reasoning behind this choice so you feel completely confident in the plan.
Other procedures we may consider
If a free-floating fragment is the cause, we perform a straightforward removal. For roughened cartilage surfaces, we may gently smooth the area to eliminate catching. Each technique is selected based on what will give you the most reliable functional outcome with the least disruption to your routine.
Is This Approach Right for You? Suitability and Realistic Expectations
Choosing a path forward is always a shared decision. We discuss every option, its realistic timeline, and what to expect during recovery.
Factors that guide our recommendation
Your age, activity level, the exact location of the tear or fragment, and the overall condition of your cartilage all shape our advice. A young runner with a repairable tear has different priorities than someone managing early joint changes. Your personal goals remain at the centre of our discussion.
Benefits and limitations to understand
Conservative management can reduce symptoms but may not eliminate a true physical block. Arthroscopic repair offers the best chance to restore normal mechanics and protect joint structure, though it requires dedicated rehabilitation. Trimming procedures often allow a quicker return to daily tasks but require ongoing joint care. We are transparent about these trade-offs so you can plan with confidence.
Managing recovery and returning to movement
Most patients walk the same day after a procedure. Post-operative discomfort is typically manageable with standard pain relief, and swelling gradually settles over the first two weeks. Full return to sport or heavy activity usually takes several weeks, guided by our physiotherapy partners. We monitor your progress closely to ensure you regain both mobility and confidence.
Typical Recovery Timeline
| Stage | Approximate Time |
| Walking | Same day to few days |
| Office work | 1-2 weeks |
| Driving | 1-3 weeks |
| Gym | 4-8 weeks |
| Sport | 3-6 months (repair dependent) |
Recovery times vary depending on the procedure performed, the extent of the injury, and individual healing factors.

When Should You Seek Medical Advice?
If your joint jams repeatedly, or if it gets stuck and will not fully straighten, it is time to arrange an assessment. Mechanical blocks often continue to recur if the underlying cause is not addressed and waiting too long can sometimes increase wear on the surrounding surfaces.
Do not wait if episodes are becoming frequent
Recurrent catching is a clear signal. Trying to push through or repeatedly forcing the joint can aggravate the cartilage. Knowing what to do when your knee locks is simple: protect it, avoid forcing the angle, and book a specialist review. Early evaluation clarifies your options and prevents unnecessary strain.
Why specialist review matters for lasting solutions
General advice can ease symptoms, but a knee specialist addresses the root mechanical cause. Our team has extensive experience in complex presentations and joint preservation techniques. We combine NHS-grade clinical rigour with the focused attention of private practice to ensure you receive thorough, evidence-based care.
Take the Next Step: Specialist Care with Us in London
Living with a joint that catches or jams can make everyday tasks, exercise, and even simple walks feel uncertain. You do not have to manage this on your own. Effective locked knee joint treatment begins with a clear, accurate diagnosis from a team that understands exactly how your joint mechanics work.
Why patients choose our London Knee Care Clinic
We have built our reputation on listening first, diagnosing precisely, and prioritising your natural joint health wherever possible. Our lead consultant brings over fifteen years of specialist experience, combining advanced surgical skills with a strong commitment to conservative, joint-preserving techniques. You will receive care at central London facilities that are designed for comfort, efficiency, and rapid access to diagnostics.
Booking your assessment is straightforward
We know knee issues disrupt your routine, which is why we keep the booking process simple. You can book an appointment with us directly through our online scheduling system or by calling our dedicated team. We aim to see you promptly, review any existing scans, and outline a clear treatment plan during your first visit. We can assess this quickly, answer all your questions, and help you move forward without guesswork.
Your knee does not have to stay stuck
Mechanical locking is highly treatable. With the right approach, most people regain full, smooth movement and return to the activities they value. We guide you on the next steps from diagnosis through recovery, ensuring you feel supported and informed at every stage.
If you are ready to discuss your symptoms and explore your options, please get in touch with our team to arrange a consultation at a time that suits your schedule. You can also schedule your consultation directly here to secure a prompt assessment. We look forward to helping you move freely again.
Frequently Asked Questions About Locked Knee Joint Treatment
Can a locked knee unlock itself?
Sometimes it can. If the blockage shifts position, your knee may suddenly regain movement. However, this does not mean the underlying problem has healed. Conditions such as a bucket handle meniscus tear or a loose body inside the joint can continue to cause recurring episodes. Even if your knee unlocks, it is important to have it assessed to identify the cause and prevent further joint damage.
Is a locked knee always a meniscus tear?
No. While a displaced meniscus tear is one of the most common causes of a true locked knee, other conditions can produce similar symptoms. These include loose fragments of cartilage or bone, scar tissue following previous surgery, cartilage flaps, and certain ligament injuries. A thorough examination and MRI scan are often needed to confirm the exact diagnosis.
Can physiotherapy fix a locked knee?
It depends on the cause. Physiotherapy can be very effective when symptoms are due to muscle weakness, joint stiffness, inflammation, or pseudo-locking caused by pain and muscle spasm. However, if there is a true mechanical block inside the joint, such as a displaced meniscus tear or loose fragment, physiotherapy alone is unlikely to remove the obstruction. In these cases, specialist treatment may be required.
Is knee locking an emergency?
Not every episode of knee locking is an emergency, but a knee that suddenly becomes stuck and cannot fully straighten should be assessed promptly. Early diagnosis is particularly important if a displaced meniscus tear is suspected, as timely treatment may improve the chances of preserving the damaged tissue. You should seek urgent medical attention if locking is accompanied by severe swelling, inability to bear weight, fever, redness, or numbness.
Do I need an MRI for a locked knee?
In many cases, yes. An MRI scan is the most accurate way to assess the soft tissues inside the knee, including the meniscus, ligaments, cartilage, and other structures that may be causing the lock. While X-rays can help assess bone alignment and arthritis, they cannot show most soft tissue injuries. MRI often plays a key role in confirming the diagnosis and planning treatment.
How long should I wait before seeing a specialist?
If your knee has locked more than once, feels unstable, or will not fully straighten, it is best to seek specialist advice as soon as possible. Waiting for symptoms to settle may delay diagnosis and allow the problem to worsen. Early assessment helps identify whether conservative treatment is appropriate or whether a procedure may be needed to restore normal movement.
Can you walk on a locked knee?
Some people can still walk with a partially locked knee, while others find it extremely difficult. Walking on a mechanically locked knee may place extra stress on other parts of the joint and could worsen symptoms. If your knee is stuck, avoid forcing movement and arrange an assessment to determine the cause.
Will I need surgery for a locked knee?
Not always. Treatment depends on the underlying cause. Some cases respond well to physiotherapy, activity modification, and strengthening exercises. However, if imaging confirms a displaced meniscus tear, loose body, or another mechanical obstruction, arthroscopic keyhole surgery may be the most effective way to restore normal joint movement and relieve symptoms.