
Few things are quite as alarming as a knee that suddenly refuses to move. One moment you are bending down, getting up from a chair, or walking across a room, and the next your knee feels completely stuck. It might be painful. It might not. But either way, a locked knee is deeply unsettling, and most people have no idea what is actually causing it.
The good news is that knee locking is not a life-threatening problem, and in most cases it is very treatable once the cause is properly identified. What matters is understanding what type of locking you are dealing with, because a locked up knee joint caused by something physically stuck inside the joint is a very different situation from one caused by pain and muscle spasm. Getting that distinction right is the foundation of getting the right treatment.
This guide explains the two types of locked knee, what causes each one, what your symptoms might be telling you, and what your options are if your knee keeps locking up and is affecting your daily life.
What Does It Mean When Your Knee Locks
A locked knee is broadly defined as a knee that cannot move through its full range of motion, either because something is physically blocking it from inside the joint, or because pain and muscle tension are preventing normal movement. These two situations look similar from the outside but have completely different causes and require completely different treatment.
Understanding which type applies to you is the single most important step. Knee locking up during bending, a knee getting stuck when bending, or a knee that catches when bending and then pops free are all experiences that fall under this broad description, but the underlying reason can vary significantly.
The knee joint is designed to bend and straighten smoothly through a specific range of movement. When something disrupts that smooth movement, whether it is a physical obstruction, inflammation, or muscle spasm, the result is a knee that feels stuck, restricted, or mechanically unreliable. My knee keeps locking up is one of the most common complaints we hear from patients, and in almost every case, a proper assessment quickly identifies the cause and a clear path forward.
True Locked Knee Versus Pseudo Locked Knee
This is the most important distinction in understanding why your knee is locking, and it is one that many patients never hear explained clearly before they come to see us.
What Is a True Locked Knee
A true locked knee occurs when something inside the knee joint physically prevents it from moving. The joint is mechanically blocked, not just painful or stiff. The most characteristic feature of true mechanical knee locking is that it typically prevents the knee from fully straightening rather than bending. You can usually bend the knee to some degree, but you cannot get it completely straight. The leg may be held in a slightly bent position, and trying to force it straight produces sharp resistance rather than gradual stiffness.
True locking is less common than pseudo locking but tends to be more significant when it does occur. The knee is not choosing to stay bent because of pain. Something is physically in the way inside the joint, and that obstruction needs to be identified and addressed.
What Is a Pseudo Locked Knee
Pseudo locked knee, sometimes called false locked knee, is far more common. It occurs when severe pain or swelling around the knee triggers the surrounding muscles to go into protective spasm. The muscles tighten and contract to guard the joint against further injury, which makes bending or straightening the knee painful and very difficult, even though there is nothing physically blocking the joint from moving.
Unlike true locking, pseudo locking can restrict both bending and straightening rather than just extension. The knee is not genuinely mechanically stuck. It is being held in place by the body’s own protective response to pain or inflammation. Once the underlying pain trigger is identified and treated, the spasm typically eases and movement returns.
Understanding this difference matters because the treatments for true and pseudo locking are very different. Treating a pseudo locked knee like a true locked knee, or vice versa, leads to unnecessary procedures or delayed recovery.
Locked Knee Symptoms to Recognise
Locked knee symptoms can vary depending on whether the locking is true or pseudo, and depending on the underlying cause. However, there are common patterns that help identify what is happening.
The most common symptoms include the following.
- The knee feels physically stuck in one position and resists movement beyond a certain point
- Knee locking and pain occurring together, particularly when trying to straighten or fully bend the joint
- Knee locking and swelling appearing together, with the joint looking visibly larger than normal
- A sensation of knee clicking and locking, where you feel or hear something catching inside the joint before it frees up
- Knee locking when straightening after a period of bending, such as when standing up from a chair
- Sharp pain when the knee locks, particularly if a fragment is catching between the joint surfaces
- Knee locking at night, waking you from sleep or making it difficult to find a comfortable position
- Knee giving way and locking together, suggesting significant instability inside the joint
It is worth noting that a knee that catches and then frees itself, sometimes with a pop or click, is a different experience from a knee that stays locked until it is gently manipulated back. Both are worth investigating, but a knee that stays locked is generally more urgent. If your knee locks and will not straighten at all, this warrants prompt specialist assessment rather than waiting to see if it resolves on its own.

Locked Knee Causes and What Is Getting in the Way
What causes a knee to lock depends on whether the locking is true or pseudo. For true locking, there is always a specific physical obstruction inside the joint. For pseudo locking, the cause is whatever is generating enough pain to trigger muscle spasm.
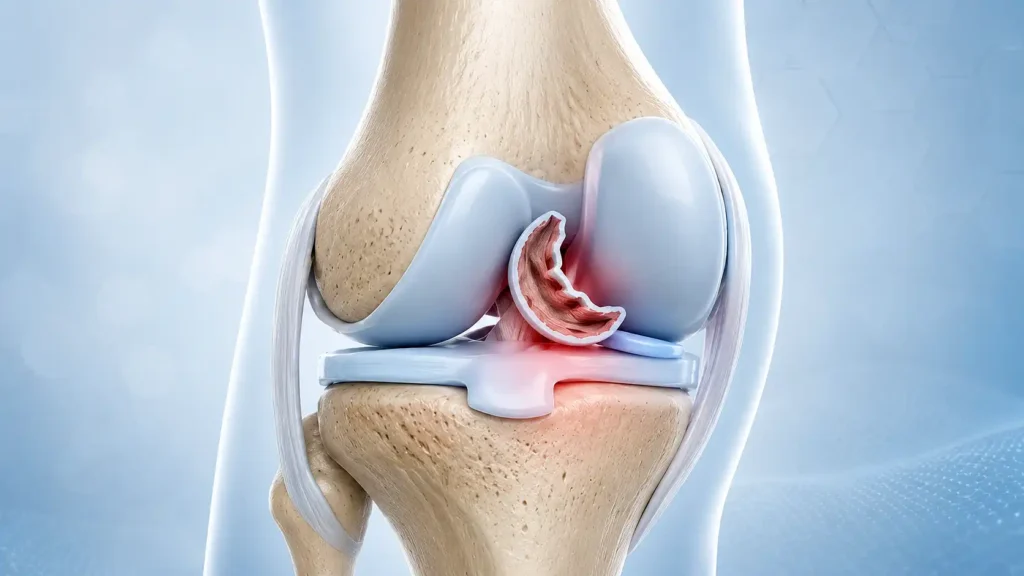
Meniscus Tear and Knee Locking
A meniscal tear is by far the most common cause of true locked knee. The meniscus is a C-shaped piece of cartilage that sits between the bones of the knee and acts as a shock absorber. When it tears, a portion of the torn tissue can flip into the centre of the joint and become wedged there, physically preventing the knee from straightening. This specific pattern is called a bucket handle tear, named because the torn segment of cartilage flips inward like the handle of a bucket.
A bucket handle tear of the meniscus tends to produce a sudden onset of locking, often following a twisting injury, and is usually accompanied by significant pain and swelling. It is one of the clearest presentations of true mechanical knee locking and is one of the most common reasons we arrange keyhole surgery to resolve a locked knee. Meniscus tear knee locking of this type rarely resolves without surgical treatment because the flipped fragment cannot find its way back into position reliably on its own.
Loose Body in the Knee Joint
A loose body is a small fragment of bone or cartilage that has broken away from the joint surface and floats freely inside the knee. When this fragment drifts into the wrong place, it can get wedged between the joint surfaces and cause the knee to lock suddenly. Loose body knee locking tends to be unpredictable, appearing and disappearing as the fragment moves around inside the joint. The knee may lock in one episode and then move freely again for days or weeks before the next episode.
Loose bodies can develop following an injury, from a condition called osteochondritis dissecans where a section of bone and cartilage separates from the joint surface, or from osteoarthritis where pieces of damaged cartilage break away over time. Cartilage fragment knee joint problems of this type are more common in older patients but osteochondritis dissecans is particularly seen in active teenagers and young adults.
Plica Syndrome and Knee Locking
Plica syndrome is a less commonly known cause of knee locking that often goes undiagnosed for some time. The plica is a fold of the synovial membrane, the thin lining of the knee joint, that is a normal anatomical feature in most people. In some individuals, this fold becomes thickened and irritated through overuse or injury, and begins to catch on the bony surfaces inside the joint during movement. This can produce a snapping, catching sensation and in some cases restrict movement enough to feel like locking.
Plica syndrome is most common in active individuals and is more likely to be a cause of pseudo or partial locking than true complete locking. It tends to respond well to physiotherapy in the first instance, though in cases where conservative management has not worked, keyhole surgery to release or remove the thickened plica produces reliable results.
Knee Locking and Arthritis
Knee locking arthritis is most commonly a cause of pseudo locking rather than true mechanical blocking, though it can contribute to both. In osteoarthritis, the cartilage within the joint wears down and the joint surface becomes irregular. This irregular surface can catch and cause a sensation of catching or locking during movement. Bone spurs, which develop as part of the arthritic process, can also occasionally act as loose bodies if they break away.
Rheumatoid arthritis and gout can cause severe joint inflammation and swelling that triggers muscle spasm and pseudo locking, particularly during a flare. In these cases, treating the inflammatory condition directly is the most effective way to resolve the locking episodes.
When Your Knee Locks in Specific Situations
Many patients notice that their knee locking happens in particular positions or situations rather than all the time. Understanding the pattern can help us identify the likely cause more quickly.
A knee locked in bend position, where the joint seems fixed in a slightly flexed angle and cannot be straightened, is the classic presentation of a true mechanical block, most often from a bucket handle meniscal tear or a loose body that has become wedged in extension.
Knee locking when kneeling is often linked to plica syndrome, a loose body, or meniscal damage, since kneeling places specific compressive and rotational forces on the joint that can cause an internal fragment to shift into a blocking position.
Locked knee standing is a common and particularly frustrating pattern, where the knee feels stuck or unreliable when bearing full weight in a standing position. This can be associated with both true and pseudo locking, since weight bearing increases the compressive forces inside the joint and can either physically wedge a loose fragment or trigger pain-related spasm.
Knee keeps locking up when walking is one of the most common presentations we see. Intermittent locking during walking, where the knee catches or briefly restricts and then frees up again, is often caused by a loose body or a partially torn meniscal flap that intermittently shifts in and out of the joint space.
Knee locks up in cold weather is something many patients notice and wonder about. Cold temperatures reduce the viscosity of the synovial fluid that lubricates the joint, making movement slightly stiffer and less fluid. In a knee that already has an internal problem, this reduction in fluid mobility can make locking episodes more frequent or more pronounced in colder conditions, particularly first thing in the morning or after sitting still for a long period.
How We Diagnose a Locked Knee
Diagnosing the cause of knee locking starts with a thorough clinical assessment. We will ask you to describe exactly what happens when your knee locks, whether it blocks bending, straightening, or both, how long it stays locked, whether it frees up with gentle movement or stays fixed, and whether there was a specific injury or onset event.
A careful physical examination of the knee allows us to assess range of movement, identify the location of any tenderness, and test for specific signs that point toward meniscal damage, loose bodies, or other structural problems.
A locked knee x-ray is usually arranged first to look for loose bony fragments, bone spurs, signs of arthritis, and any structural abnormalities in the joint. However, an MRI for locked knee is far more informative for soft tissue structures. An MRI allows us to see the meniscus in detail, identify whether a bucket handle tear has occurred, locate any loose bodies that are not visible on X-ray, and assess the cartilage surfaces and ligaments at the same time. This combination of clinical assessment and appropriate imaging gives us a precise picture of what is happening inside your joint before any treatment decision is made.
Locked Knee Management and Treatment Options
Locked knee management depends entirely on whether the locking is true or pseudo, and what is causing it. There is no single treatment approach that works for every locked knee, which is why accurate diagnosis is so essential before any treatment is planned.
For pseudo locked knee caused by pain, swelling, or inflammation, the priority is addressing the underlying source of the pain. This may involve rest, ice, anti-inflammatory medication, compression, and elevation in the acute phase. Once the immediate pain and swelling have settled, physiotherapy for locked knee addresses the muscle weakness and movement restriction that often persist after the initial episode. Physiotherapy focuses on restoring normal range of movement, strengthening the muscles around the knee to improve joint stability, and addressing any biomechanical factors that may be contributing.
For true locked knee caused by a meniscal tear or loose body, physiotherapy alone is usually not sufficient. If the knee is being physically blocked by a trapped fragment of tissue or bone, the obstruction needs to be removed or repositioned before normal movement can return.
How to unlock a locked knee at home when the joint is caught in a specific position involves gentle, slow movement of the knee in the opposite direction to the block, combined with small rotating or waggling movements. In many cases of intermittent locking from a loose body, gentle manipulation of the leg in this way encourages the fragment to shift out of the blocking position, which frees the joint temporarily. However, this does not treat the underlying problem, and the locking will recur until the fragment is properly dealt with.
Keyhole Surgery for Locked Knee
Keyhole surgery is the most common and most effective treatment for true mechanical knee locking caused by a meniscal tear or loose body. The procedure involves inserting a small camera and fine surgical instruments through tiny incisions around the knee, allowing the surgeon to see inside the joint and address the problem directly.
For meniscus surgery knee locking caused by a bucket handle tear, the torn flap of cartilage is either repaired and sutured back into position, or the unstable portion is trimmed away depending on the size, location, and quality of the tear. Loose body removal from the knee involves locating the fragment or fragments inside the joint and extracting them through the keyhole incisions. Both procedures are typically performed as day cases, with most patients going home the same day.
Recovery after keyhole surgery for knee locking is generally straightforward. Most patients are walking within a few days and return to normal daily activities within two to four weeks. A structured physiotherapy programme in the weeks after surgery helps restore full strength and confidence in the knee.
When You Should Not Wait to Get Your Knee Assessed
Some knee symptoms are safe to monitor for a short period before booking an appointment. A locked knee is generally not one of them, particularly if any of the following apply to you.
You should seek specialist assessment promptly if your knee has locked and will not straighten at all, if the locking is happening with increasing frequency, if you have significant swelling alongside the locking, or if you have heard or felt a pop inside the knee at the moment the locking began. A knee that locks completely and does not free up with gentle movement within a few minutes warrants same-day medical assessment rather than waiting for a routine appointment.
If your knee locking is accompanied by the sensation of giving way, significant instability during walking, or you are struggling with daily activities as a result, these are all signs that something inside the joint needs investigation rather than rest alone.

Expert Locked Knee Care at London Knee Care
If your knee is locking, catching, or getting stuck when bending and you want a clear answer about what is causing it and what can be done, we are here to help. As a locked knee specialist London patients trust for prompt assessment, we see patients at all stages of this problem, from intermittent catching that has been happening for weeks, to complete locking that has just occurred and is causing significant distress.
We take the time to understand exactly what your knee is doing, when it happens, what triggers it, and what your daily life and activity goals are. This shapes both the diagnostic pathway and the treatment plan we recommend. We do not take a one-size-fits-all approach, because locked knee causes vary too significantly for that to produce good outcomes.
Our clinic is led by Mr Raghbir Khakha, a consultant orthopaedic surgeon with over fifteen years of specialist experience in complex knee conditions including meniscal tears, cartilage damage, loose body removal, and keyhole surgery. He takes a careful, patient-focused approach to every case, explaining your findings clearly and giving you honest advice about your options and realistic outcomes.
You can book your consultation directly online at a time that suits you. If you would prefer to speak with our team first or have any questions before booking, please contact us and we will help you work out the most appropriate next step for your knee.
Frequently Asked Questions
Why does my knee lock when I bend it?
The most common reasons are a torn piece of meniscal cartilage that catches inside the joint during bending, a loose body that shifts into a blocking position, or severe pain and swelling triggering the surrounding muscles to spasm and restrict movement. The pattern of your locking, whether it blocks bending, straightening, or both, and whether it frees up on its own or stays fixed, helps point toward the specific cause.
Is knee locking bad?
Yes, persistent or recurring knee locking is a sign that something inside the joint needs attention. Occasional mild catching that resolves quickly may be less urgent, but a knee that locks completely and cannot be straightened, or that is locking with increasing frequency, should not be left without proper assessment. Leaving the underlying cause untreated risks further damage to the joint structures over time.
My knee keeps locking up, what should I do?
If your knee is locking repeatedly, the first step is to get a proper diagnosis rather than continuing to manage each episode at home. Recurring locking almost always means there is a specific structural problem inside the joint that is not going to resolve on its own. Book a specialist assessment, bring a description of when and how the locking happens, and we can arrange the appropriate imaging to identify the cause and plan the right treatment.
Knee locks up when bent then pops, what does this mean?
A knee that locks when bent and then frees with a pop is a very common presentation of a loose body inside the joint. The fragment drifts into a position where it blocks movement, and the pop you feel or hear is the fragment shifting back out of the way as the joint moves. This pattern tends to recur and become more frequent over time, and the fragment can occasionally shift into a position where it does not free up easily, which is why it is worth having it assessed before that happens.
Why is my knee locking up and popping?
Locking combined with popping most commonly points toward a loose body, a partially torn meniscal flap, or plica syndrome. The pop is the sound or sensation of a fragment or thickened tissue shifting position inside the joint. If the popping is associated with pain or swelling, or if the locking episodes are becoming more frequent, a specialist assessment and MRI will clarify exactly what is happening.
Locked knee pass out, is this related?
Fainting or feeling faint alongside a locked knee episode is not caused by the knee locking itself. What typically happens is that sudden, severe pain from a locking episode triggers a vasovagal response, an automatic nervous system reaction where blood pressure drops briefly in response to acute pain or shock. This can cause dizziness, sweating, nausea, and occasionally fainting. It is generally harmless and resolves quickly once the pain eases. However, if you are regularly fainting or feeling faint alongside knee symptoms, it is worth mentioning to your doctor to rule out any other contributing factors unrelated to the knee.
Knee locks up in cold weather, why?
Cold temperatures reduce the viscosity of the synovial fluid that lubricates your knee joint, making movement slightly stiffer and less fluid than in warmer conditions. In a knee that already has an underlying problem such as a loose body or meniscal damage, this reduction in joint lubrication efficiency can make locking episodes more likely, particularly first thing in the morning or after sitting still for a long period in the cold. It is not the cold causing the underlying problem, but it can make an existing problem more symptomatic.
Should I go to A and E for a locked knee?
If your knee has locked completely and you cannot straighten it at all, if you are in severe pain, or if the locking happened after a significant injury such as a fall or collision, then yes, same-day assessment is appropriate, either through A and E or an urgent care centre. If your knee is catching and occasionally locking but you can still move it to some degree and the pain is manageable, booking a prompt specialist appointment is the right course of action rather than waiting in A and E.
Can knee locking be permanent?
In cases of true locked knee caused by a trapped meniscal fragment or loose body, the locking will not resolve permanently on its own without treatment. The fragment may shift and free the knee temporarily, but it will continue to cause intermittent locking until it is removed or repaired surgically. Pseudo locked knee caused by pain and spasm does resolve once the underlying pain source is treated, and is not a permanent condition in the way true mechanical locking can be.
Why does my knee catch when bending?
A knee that catches when bending, where you feel a brief resistance or snapping sensation during movement, is often caused by a loose body or a partially torn meniscal flap catching between the joint surfaces momentarily during flexion. Plica syndrome can produce a similar catching or snapping sensation. Catching that is becoming more frequent, more painful, or that is progressing to full locking episodes warrants a specialist assessment to identify and address the underlying cause before it worsens.
Is knee locking serious?
Knee locking is a significant symptom that indicates something inside the joint needs attention. It is not dangerous in an immediately life-threatening sense, but it is a sign of a structural problem that will not resolve without proper diagnosis and treatment. A knee that locks repeatedly and is left without assessment risks progressive joint damage, particularly if a loose body or meniscal fragment is repeatedly catching on the cartilage surfaces with each episode.



